
Abstract
Human metapneumovirus is an emerging human respiratory pathogen first discovered in 2001. It clinically resembles respiratory syncytial virus, can cause both upper and lower tract disease, and has been associated with serious illness in the young, among the immunosuppressed, and in the chronically ill. Cough and congestion are frequently reported, and respiratory failure may occur. Initial infection occurs during early childhood, and repeated infections throughout life impart only transient immunity. Diagnosis is by reverse transcription-polymerase chain reaction or rising serologic titers. No commercial laboratory tests or treatments are available. Primary care physicians should maintain vigilance for outbreaks of newly discovered and emerging respiratory illnesses.
Acute respiratory tract infections (ARIs) are important causes of illness and mortality worldwide. In the United States, ARIs are the sixth leading cause of death and account for more than half a million hospital admissions and 8 to 10 million outpatient visits per year.1,2 The bacterial or viral agent responsible for an ARI is often uncertain. In 40% to 60% of community-acquired pneumonias, the pathogenic agent remains undetermined.3 A similar situation exists with ARIs that are presumed to be viral.4–9 Two or more causative agents probably occur more frequently than are currently documented.
Recent progress in epidemiologic surveillance and molecular biology has allowed the rapid recognition and identification of several newly emerging respiratory pathogens. In the last decade, the bird flu (avian influenza A, H5 N1), severe acute respiratory syndrome (SARS) coronavirus, and human metapneumovirus (HMPV) have been discovered, their viruses isolated, and clinical data from infected patients compiled and published. Recent research indicates that HMPV is the cause of an important proportion of acute upper and lower respiratory tract infections in all age groups.10–13
The Virus
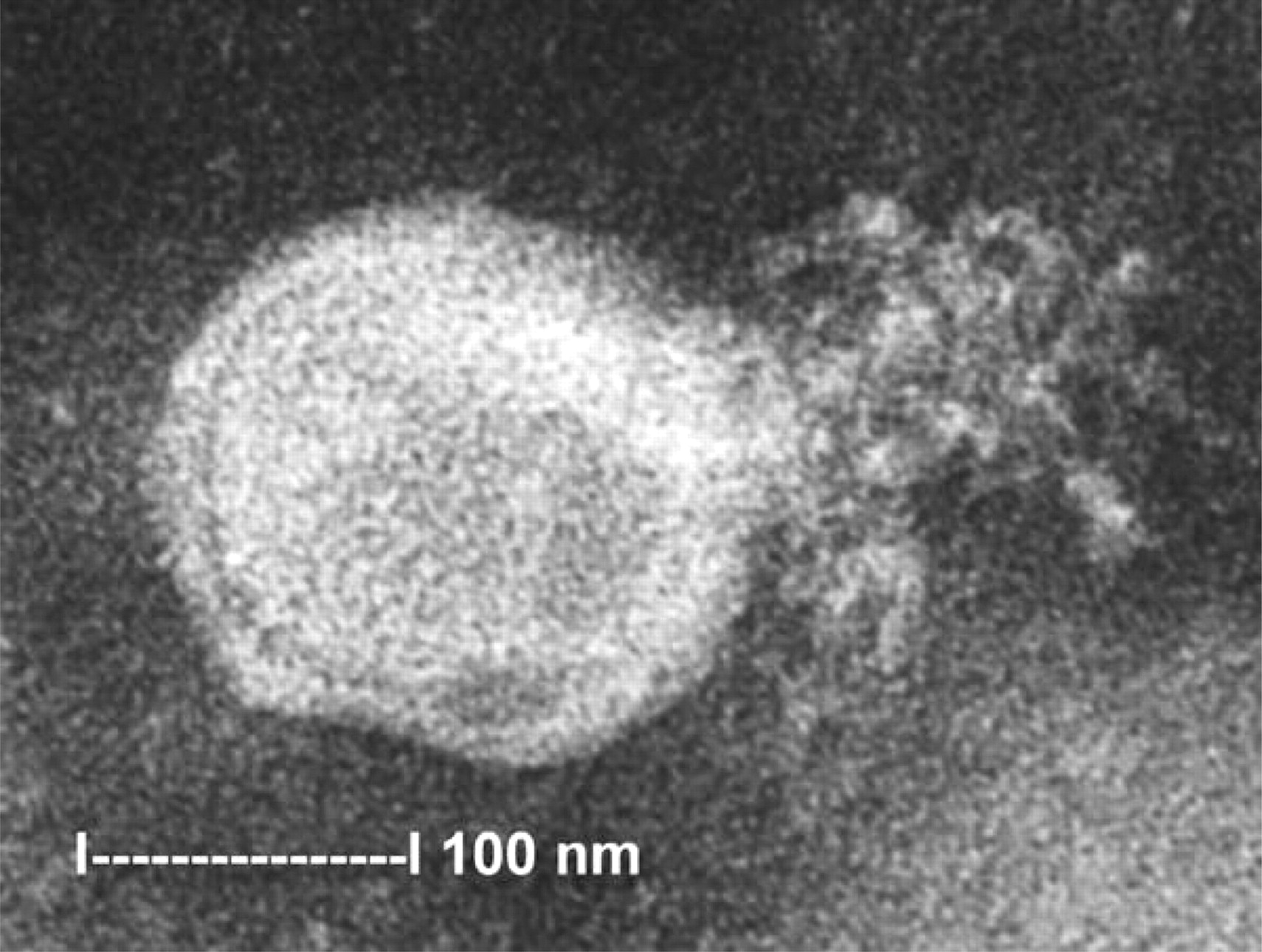
In 2001, a new respiratory tract viral pathogen, human metapneumovirus, was first reported from the Netherlands.11 The virus was identified in 28 stored nasopharyngeal aspirates collected over a 20-year period. Its discovery may have been delayed because the virus replicates poorly on routinely used continuous cell lines. Using random arbitrarily primed-polymerase chain reaction, the virus was found to be in the Paramyxoviridae family, the first human pathogen of the genus Metapneumovirus. Both respiratory syncytial (RSV) and parainfluenza viruses are paramyxoviruses and are well known to clinicians. An indirect immunofluorescent antibody test was developed that allows serologic diagnosis. With the virus identified and a serologic test available, researchers have begun exploring the epidemiology and clinical presentations of the disease. It occurs in seasonal outbreaks that seem to coincide with RSV season.10,13 The incubation period was 5 to 6 days based on a single documented hospital-acquired infection.5 An attempt to identify the virus in 400 healthy children under 2 years of age was unsuccessful,11 although asymptomatic and carrier states have been reported in children and adults.10,12 Because most descriptions of clinical signs and symptoms are based on studies of children ill enough to require hospitalization, a true picture of the pathogenicity of HMPV is still emerging (Figure 1).
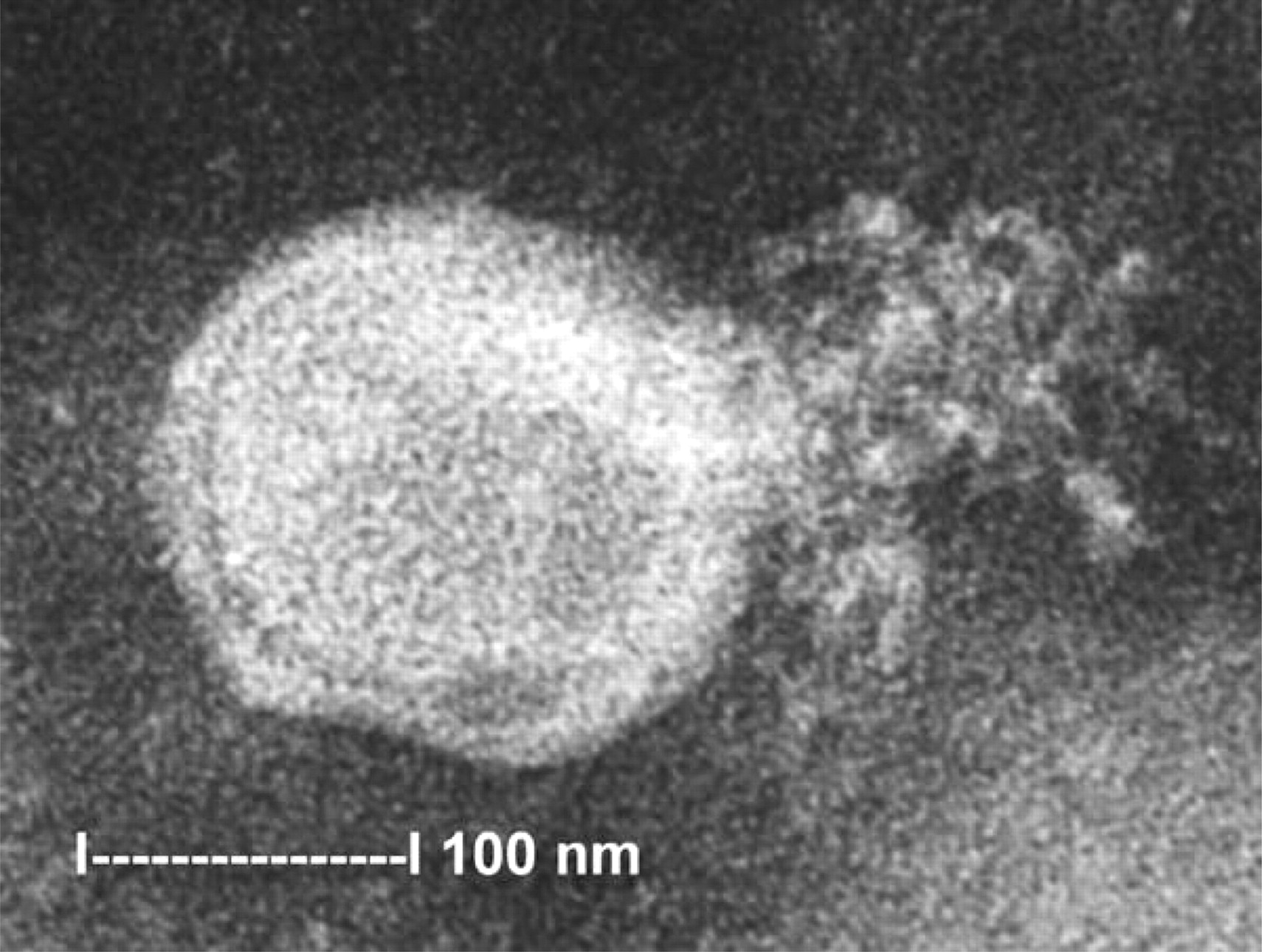
Electron micrograph of human metapneumovirus collected from the supernatant of rhesus monkey kidney (LLC-MK2) cell culture. A virion-releasing nucleocapsid is shown. [Reprinted from Chan PK, Tam JS, Lam G-W, et al. Human metapneumovirus detection in patients with severe acute respiratory syndrome. Emerg Infect Dis 2003;9:1058–63].
Epidemiology
The HMPV has been reported worldwide. One hundred percent of 72 stored serum samples from children and adults collected in 1958 were positive for HMPV, indicating that the virus has been circulating in human populations for years.11 Seroprevalence increased from 25% in children between 6 months and 1 year old to 100% in those over 5 years of age.11 There are at least 2 different genetic lineages, and viral genome heterogeneity may also allow for incomplete immunity and repeated infections.10,14,15 Human metapneumovirus infection accounts for approximately 2% to 12% of pediatric lower respiratory illnesses and a lesser percentage in adults.4–10,12,13,15–18 Antibody titers in children increased with age, which suggests boosting of antibody response.11
Clinical Features in Children
In infants and children, lower respiratory tract illness caused by HMPV is similar to other viral-associated bronchiolitis and cannot clinically be distinguished from the RSV, influenza, and parainfluenza viruses. Cough was reported in more than 90% of children; more than 75% had rhinorrhea, and more than 50% had fever.4–10,13,16 An exacerbation of existing asthma or wheezing was present in about one half. Hypoxia and abnormal chest radiograph findings were common in hospitalized patients; perihilar infiltrates, peribronchial thickening, and air trapping were reported.13 Found less frequently were otitis media, diarrhea, rash, conjunctivitis, and febrile seizures.5,7 Most infants and children received a discharge diagnosis of bronchiolitis, croup, pneumonia, bronchitis, or asthma exacerbation (in decreasing order of frequency).7,10,15,16 Co-infection with other respiratory viruses occurs, and simultaneous infection with HMPV and RSV has been postulated to cause severe disease, often requiring intensive care admission and ventilatory support.17 The disease is believed to more serious in infants and in those with chronic illnesses,18 and one death in an immunocompromised child has been reported.19 Primary infection with the virus is believed to cause the most severe symptoms.
Few articles have reported laboratory data. One report of 32 hospitalized children under the age of 18 months noted that 29% had lymphopenia and 6% had elevated transaminases.5 In another series of 10 hospitalized children, normal white blood cell counts and elevated C-reactive protein levels were reported.8
Adult Disease
Several community studies in adults have helped to define the role of HMPV as the cause of ambulatory ARIs.12,20 Two longitudinal studies, one conducted in British general practices over a single winter20 and the other in adults in Rochester, New York, over 2 winter seasons,12 reported HMPV infection rates of 2.2% and 1.5%/7.0%, respectively. In the majority of healthy young and elderly adults, HMPV was predominately a mild disease characterized by cough, hoarseness, congestion, and rhinorrhea.12 Sore throat, hoarseness, sputum production, and constitutional symptoms were present in more than half of patients. Fever was unusual. Immunocompromised and chronically ill patients often require hospitalization.12,21 No laboratory results of adults with HMPV have been reported. Treatment has been supportive.
The HMPV is not the pathogenic agent responsible for Severe Acute Respiratory Syndrome (SARS). But the 2 illnesses overlap in their signs and symptoms. Of interest is a report that 40% of 48 patients admitted to a Hong Kong hospital with suspected SARS were infected with HMPV alone, and 12% had HMPV plus SARS coronavirus. Only 10% had the SARS virus alone.22 A similar finding has been reported from Toronto.23 A 40-year-old man who met the World Health Organization’s criteria for probable SARS was discovered at postmortem examination to have died of HMPV pneumonitis.24
Conclusions
The newly discovered human metapneumovirus is an important cause of community-acquired acute respiratory infections in infants, children, and adults. Both the upper and lower respiratory tracts may be involved, and serious illness may occur in the very young and in those who are chronically ill or immunosuppressed. Further research should answer the many questions about HMPV.
The increased interest in respiratory pathogens, coupled with heightened surveillance and improved laboratory methods, will lead to the discovery of new pathogenic agents causing pneumonia-like illness. Up-to-date knowledge and heightened awareness by primary care physicians are essential in the recognition of new diseases or patterns of disease because we are the first line of defense in Public Health efforts to limit the epidemic spread of emerging pathogens.
Acknowledgments
I appreciate the technical assistance from Colleen Flewelling and Donal Gordon.
- Received for publication August 5, 2004.
- Revision received August 5, 2004.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.