
Subacromial septic bursitis after corticosteroid injection is exceedingly rare. This report describes a case of Staphylococcus aureus subacromial septic bursitis after corticosteroid injection in a patient undergoing isotretinoin (Accutane) therapy. This case is only the third reported in the literature linking a corticosteroid injection with septic subacromial bursitis1,2 and the first to describe an association with isotretinoin therapy.
Isotretinoin is an established treatment of severe nodulocystic acne and a variety of dermatologic conditions.3 Infectious complications from isotretinoin are rare. However, increased S aureus colonization of the nasal mucosa and skin is well established,4 and cases of S aureus infection associated with isotretinoin therapy are reported.5,6 Isotretinoin should be recognized as a risk factor for developing infections such as septic bursitis after percutaneous injection. Physicians performing these injections should be aware of this uncommon complication.
Case Reports
A 55-year-old woman presented for evaluation of right shoulder pain. The patient awoke with spontaneous onset of severe shoulder pain 1 day before her evaluation. She denied any antecedent trauma, injury, or change in activity. The pain was anterior and worse with any attempt of shoulder movement. She denied prior shoulder problems, neck or periscapular pain, numbness, tingling, or weakness in her upper extremities, fever, or recent illness.
Her past medical history was unremarkable except for adult nodulocystic acne for which she had been taking isotretinoin (1 mg/kg/d) for the past 6 months. She was on no other medications and did not smoke or drink alcohol. She was a competitive runner who exercised daily and was in excellent condition.
Physical examination revealed a thin, well-developed woman with a temperature of 97.5°C and blood pressure of 120/80 mm/Hg. Patient had guarded right shoulder movements but otherwise was in no distress. Inspection of her right shoulder revealed no muscle atrophy, erythema, or swelling. Active range of motion (ROM) was limited to 30° of flexion and 30° abduction secondary to pain. She had full passive ROM in flexion, abduction, and external rotation symmetric with her left shoulder. Neer impingement test was negative, but Hawkins impingement test was positive. Strength of abduction or external rotation with the elbow at her side was 5-/5 but decreased to 4-/5 because of pain with any amount of flexion or abduction of the arm. She was tender over the anterior soft tissues and anterior rotator cuff but had no tenderness of the biceps long-head tendon or warmth to palpation. She had full active ROM of the cervical spine, and her distal neurologic examination was normal in the C5–T1 distributions.
A presumptive diagnosis of acute subacromial bursitis or calcific tendinitis was made, and a subacromial corticosteroid injection performed using aseptic technique and a posterolateral approach. The skin was prepped with betadine and alcohol and a mixture of 8 mL of 1% lidocaine and 1 mL of methylprednisolone 80 mg/mL was injected into the subacromial space without difficulty. A sterile syringe and previously unopened bottles of medications were used. Shortly after the injection, the patient had improved pain and active movement of her shoulder. Radiographs were not immediately available in the office but were taken later that day and were normal.
The patient improved dramatically for 72 hours. Four days after her injection, while traveling out of state, she presented to an emergency department complaining of anterior right shoulder pain, redness, swelling, and warmth. Labs revealed an elevated erythrocyte sedimentation rate (ESR) of 60 (reference range, 0 to 25 mm/hour) and a normal white blood cell count. Repeat radiographs were normal. She was treated with one dose of intramuscular ceftriaxone and sent home on oral prednisone and cephalexin (500 mg every 6 hours).
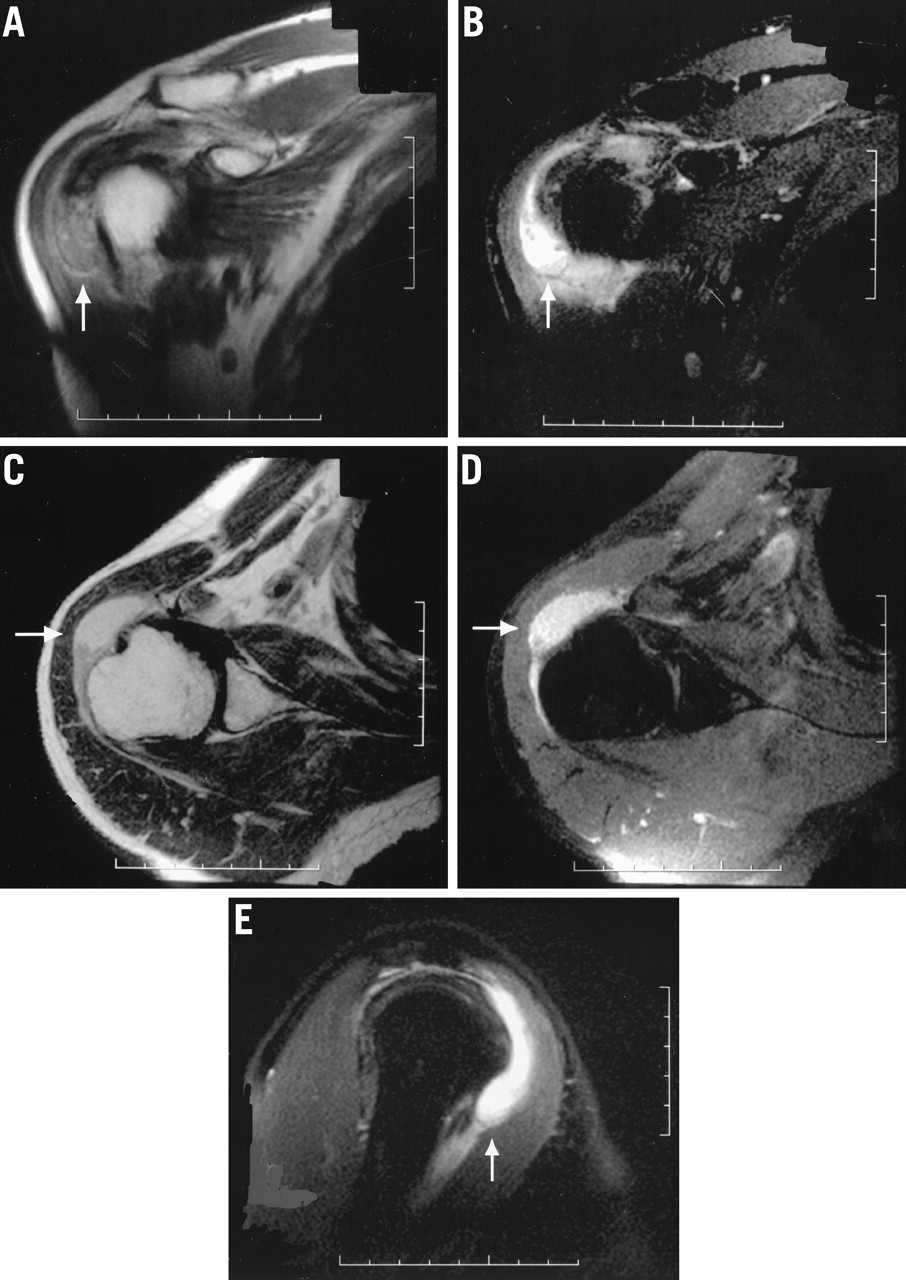
She returned to our clinic 8 days after her initial evaluation feeling slightly better. Examination revealed mild warmth, swelling, and subtle anterior fluctuance without erythema. Magnetic resonance imaging (MRI) demonstrated mild supraspinatus tendinosis without tear and a moderate subacromial/subdeltoid fluid collection without extension into the glenohumeral joint suggestive of “bursitis” (Figure 1). Needle aspiration of the anterior fluid collection drained 3 mL of grossly purulent fluid. Gram-stain revealed rare intracellular Grampositive cocci, fluid white blood cell count over 120,000/μL, and culture grew S aureus.

MRI of the right shoulder demonstrates a moderate sized subacromial/subdeltoid fluid collection (arrow) without extension into the glenohumeral joint. There is also mild surrounding soft tissue edema. A: coronal T1. B: coronal T2. C: axial T1. D: axial T2. E: sagittal T2.
Repeat MRI 1 day later showed a slight decrease in subacromial fluid collection. The patient was followed closely; by day 10 of oral antibiotics, she was pain-free with full active range of motion and strength. Her ESR decreased to 21. She received a total of 14 days of cephalexin and at more than 1 year of follow-up is still doing well.
Discussion
Subacromial corticosteroid injections are an extremely common procedure performed by orthopedic, rheumatology, and primary care physicians, yet infectious complications are extraordinarily rare. Although the exact incidence of septic bursitis is unknown, review of the literature found only 20 cases1,2,7–18 of documented subacromial septic bursitis. Nearly all these cases were associated with severe underlying medical conditions, and only 2 cases1,2 occurred after a corticosteroid injection. Chartash et al1 described a 53-year-old man who developed a subdeltoid septic bursitis after intramuscular triamcinolone injections into his deltoid for contact dermatitis. Garcia-Porrua et al2 described an elderly man who developed subacromial septic bursitis after a series of 3 corticosteroid injections within a 3-week period.
Septic bursitis affects superficial bursa more commonly than deep bursa. Superficial bursa, such as the olecranon and prepatellar bursa, lie in the subcutaneous tissue and are more susceptible to infection through traumatized skin.19,20 Most cases of subacromial bursitis are reported in patients with severe underlying medical conditions that make them immunocompromised and more susceptible to infection.1,2,7–9,12,13,17,18 Other causes include hematogenous spread, trauma, and iatrogenic complications. S aureus is the most common pathogen and is found in approximately 80% of cases.1,2,7 Subacromial septic bursitis may also coexist with septic arthritis of the glenohumeral joint via communication through a partial or complete rotator cuff tear.19
Subacromial septic bursitis presents with shoulder pain, swelling, redness, and warmth. Systemic signs such as fever and an elevated white blood cell count, ESR, or C-reactive protein level may be present depending on the severity of the illness. Septic bursitis should be suspected in patients with disease states associated with immunocompromise, patients with systemic infection, and patients who have received a corticosteroid injection. MRI or ultrasound can identify fluid collections in the subacromial space and contiguous subdeltoid bursa. A large fluid collection with surrounding soft tissue edema suggesting cellulitis is consistent with a septic bursitis but should always be correlated clinically. Needle aspiration can confirm the diagnosis and identify the pathogen with appropriate analysis and culture of bursal fluid. Treatment of subacromial/subdeltoid bursitis depends on the severity of the illness and includes oral and parenteral antibiotics, needle aspiration, incision and drainage, and surgical debridement.
Isotretinoin produces clinical improvements in nodulocystic acne through a number of mechanisms resulting in a reduction in sebum production. Isotretinoin has a number of well-known mucocutaneous and systemic side effects,3,21 although infectious complications are quite rare. Leyden and James5 describe 18 patients who developed S aureus infection during or shortly after a 5-month course of isotretinoin. Infections included furuncles of the face, trunk, and thigh, folliculitis of the scalp and arm, cellulitis of the vulva, and maxillary and frontal sinusitis. Graham et al6 also described a case of S aureus endocarditis in a patient with stable aortic insufficiency undergoing isotretinoin therapy.
Alterations in nasal and skin bacterial colonization and decreased skin barrier function as a result of increased skin dryness explain the pathogenesis of S aureus infections during isotretinoin therapy. S aureus colonization of the anterior nares and of normal skin before isotretinoin treatment exists in less than 10% of isolates.4,6 During isotretinoin treatment, however, up to 70% of patients have S aureus colonization of the anterior nares, and 50% have colonization of the skin.4,6 Isotretinoin results in the reduction of Gram-negative bacteria as a result of the marked dryness of the skin and mucous membranes. This change in microenvironment and skin barrier function seems to predispose the patient to S aureus colonization. Other skin disorders involving pronounced skin dryness and inflammation also result in increased colonization with S aureus. In patients with atopic dermatitis, S aureus was isolated from 90% of lesions and 70% of clinically normal skin.22
Isotretinoin also effects the immune system. Isotretinoin has been shown in vitro to inhibit neutrophil release of inflammatory mediators23 and also to reduce natural killer cell activity in patients taking the drug.24 The role of immune system changes on clinically significant S aureus infections remains unclear.
Although we cannot say categorically that the use of isotretinoin led directly to septic bursitis in our patient, it seems highly likely that the drug played a role in our otherwise healthy patient. The absence of initial signs of infection (redness, swelling, or warmth), skin breakdown or a source for hematogenous spread, and her rapid improvement after injection, make it unlikely her initial presentation represented the first signs of septic bursitis. Iatrogenic introduction through colonized skin despite aseptic technique is a more likely explanation.
Conclusion
Isotretinoin is a predisposing risk factor for S aureus colonization and subsequent infection. Physicians performing percutaneous injections should use caution in patients on concurrent isotretinoin therapy.
- Received for publication October 28, 2004.
- Revision received October 28, 2004.
References




{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.