
Abstract
Background: Medicaid-insured asthmatic children frequently use emergency rooms (ERs). The reasons are unclear and have predominantly been studied in inner-city populations.
Methods: We used billing data and focus groups to clarify reasons for frequent ER use by Medicaid-insured children with asthma living in rural areas and 23 towns in Kansas.
Results: High ER utilization was concentrated in a small percentage of provider practices and children with asthma. Parents expressed strong preference for primary care treatment, and identified real or perceived difficulties in using primary care as the principal reasons for ER use. Difficulties included trouble contacting primary care physicians or obtaining urgent appointments, limited continuity of care, practice systems poorly adapted to patient needs, a perception that physicians preferred patients to use emergency services, and difficulties in obtaining medications. Parents were not aware of preventive measures or case management but reported high interest in these. Parents did not recall provider discussion of asthma risk factors/preventive strategies during primary care visits, although all children with high ER utilization had multiple risk factors, including exposure to high levels of household smoking.
Conclusions: Reducing ER utilization by Medicaid-insured asthmatic children depends on overcoming barriers to effective treatment in primary care and in greater attention to preventive services.
Asthma affects at least 5 million children in the United States.1 The estimated overall prevalence of 53 to 58 per 1000 children increased from approximately 35% to 75% between 1980 and 1995.2 Even these high rates are believed to underestimate the true prevalence of this serious and potentially fatal disease.2 Despite advances in therapy, the morbidity, mortality, and costs of asthma continue to increase dramatically.3,4 Current annual costs for inpatient treatment of asthma are estimated at $1.8 billion with emergency services (ER) consuming an additional $480 million.1 Treatment in these 2 settings accounts for 38% of all direct medical costs for asthma.1 The national targets for asthma care include reducing hospitalization from 60.9 to 25 per 10,000 children under age 5 years and reducing emergency department visits from 150 to 80 per 10,000 children under age 5 years by 2010.5 To achieve these targets, national guidelines (Healthy People 2010) stress 4 responsibilities for primary care: (1) avoiding or controlling factors that may exacerbate asthma (such as occupational and environmental allergens and irritants); (2) improving compliance with therapies specific to the severity of the disease; (3) objective monitoring of the disease by the patient (or family) and health care team; and (4) active patient (and/or family) participation in disease management.
In reality, the medical, personal, social, and other costs of asthma are disproportionately borne by a minority of asthmatic patients. By one estimate, 20% of asthmatic patients consume 80% of medical resources.6 Most “high-cost” asthmatic patients belong to groups with enhanced vulnerabilities to the disease and/or greater barriers to effective management of asthma. Medicaid-eligible children are among those most vulnerable to asthma and most likely to suffer poor outcomes from the disease. Asthma is endemic in children eligible for Medicaid7, and these children have high rates of hospitalization and ER use.8 Their high utilization rates have been attributed to complex interactions between genetic predispositions, psychosocial factors, socioeconomic status, environmental exposures (including household smoking), and arrangements for medical care.6 This complexity makes asthma care in Medicaid-insured children difficult to study using conventional research designs that tend to focus on one aspect of the problem. In addition, most studies have involved children living in inner-city areas and have not had a primary care focus.
This study aimed to clarify the reasons for frequent ER use by Medicaid-insured children with asthma living in rural areas and 23 towns in Kansas as a first step in identifying primary care activities with the potential to reduce such use. The study integrated quantitative data from hospital and ER utilization patterns of these children (using a cross-sectional epidemiologic design) with qualitative information from parental focus groups to learn more about the multiple factors contributing to this complex topic.
Methods
The study population was all 2767 children (aged 0 to 17 years) insured by one Medicaid insurer in Kansas (Table 1). These children lived in unincorporated areas (4 urban areas and 19 small towns, each less than 4000 population). The 8 counties covered by this insurer represent a range of demographic characteristics and all were designated as underserved for primary care (Table 2). Medical services were provided by 53 health providers, grouped in 12 primary care practices. Ten of these practices served 20 or more patients, whereas 2 served fewer than 20 patients.
Medicaid-Insured Children in the Eight Counties Covered (n = 2767)
Selected Demographic Characteristics of Counties
All asthma-related billings for inpatient or ER services between April 1996 and May 1997 were accessed and reviewed. The data were analyzed using SAS 8.1 to provide unduplicated ER and inpatient rates using the enrolled population as the denominator. This provided the number of ER visits and hospitalizations per 10,000 enrolled children. Children were also stratified by age, and rates were calculated for children younger than 5 years.
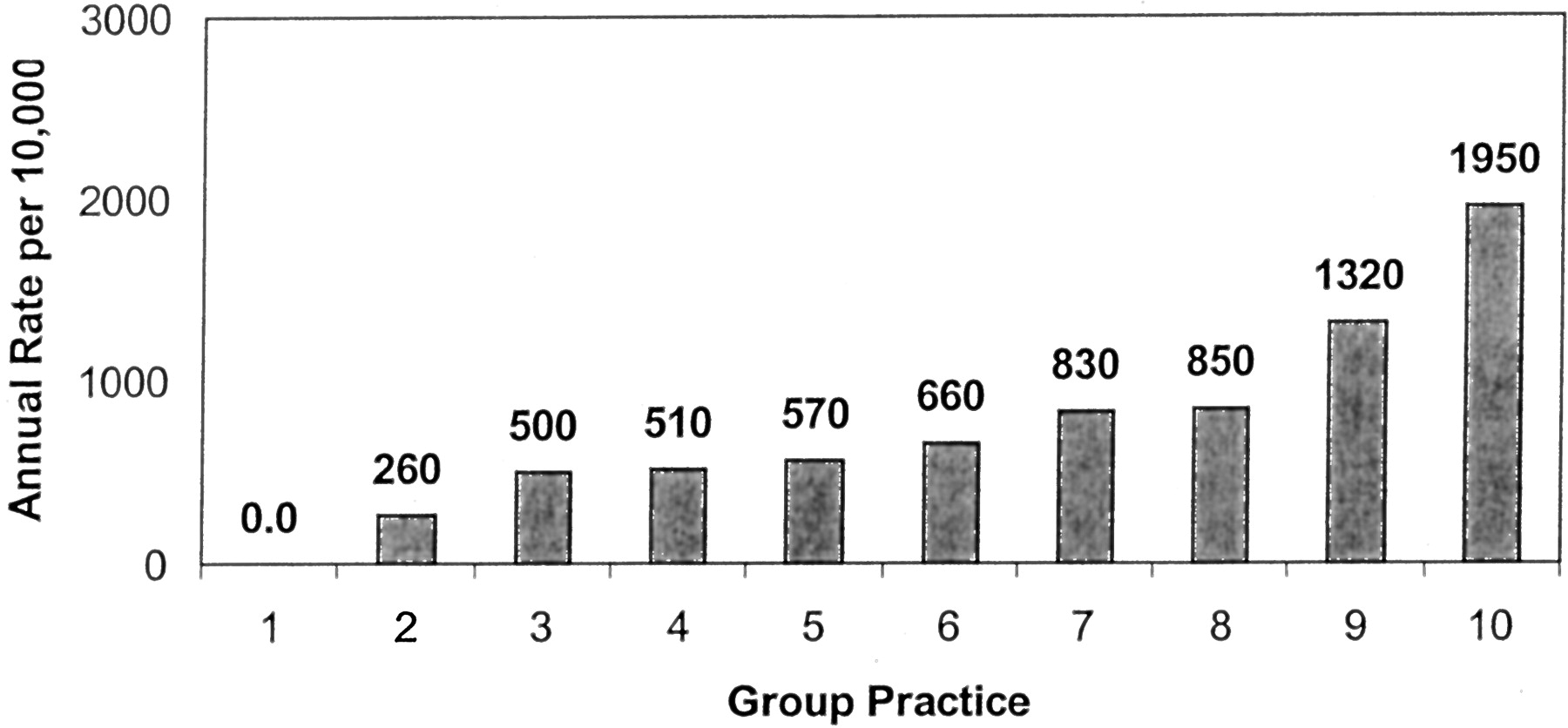
Stratified analyses were used to calculate ER utilization rates by assigned primary care physician practice for the 10 practices with more than 20 childhood Medicaid enrollees (Figure 1). ER and inpatient hospital utilization by individual children (the number of children per 10,000 enrollees who ever used the ER or were hospitalized) were also calculated. The parents of children with ER visits resulting in hospitalization or multiple asthma-related emergency department visits were invited to participate in focus groups to provide the patient-family perspective on the beliefs and motivations underlying the choice of ER. The 2-hour focus group sessions were conducted at a community center. Participants were provided with transportation, childcare, refreshments, and a $10 voucher inducement to attend. The commitment to attend was confirmed by a telephone reminder on the day of the meeting. The focus group session followed an open-ended script to prompt discussion of asthma knowledge, related family behaviors, physician practices, and experiences with health care systems related to the child’s asthma. Participant input was recorded and consensus opinions transcribed by one of the authors (DDF).
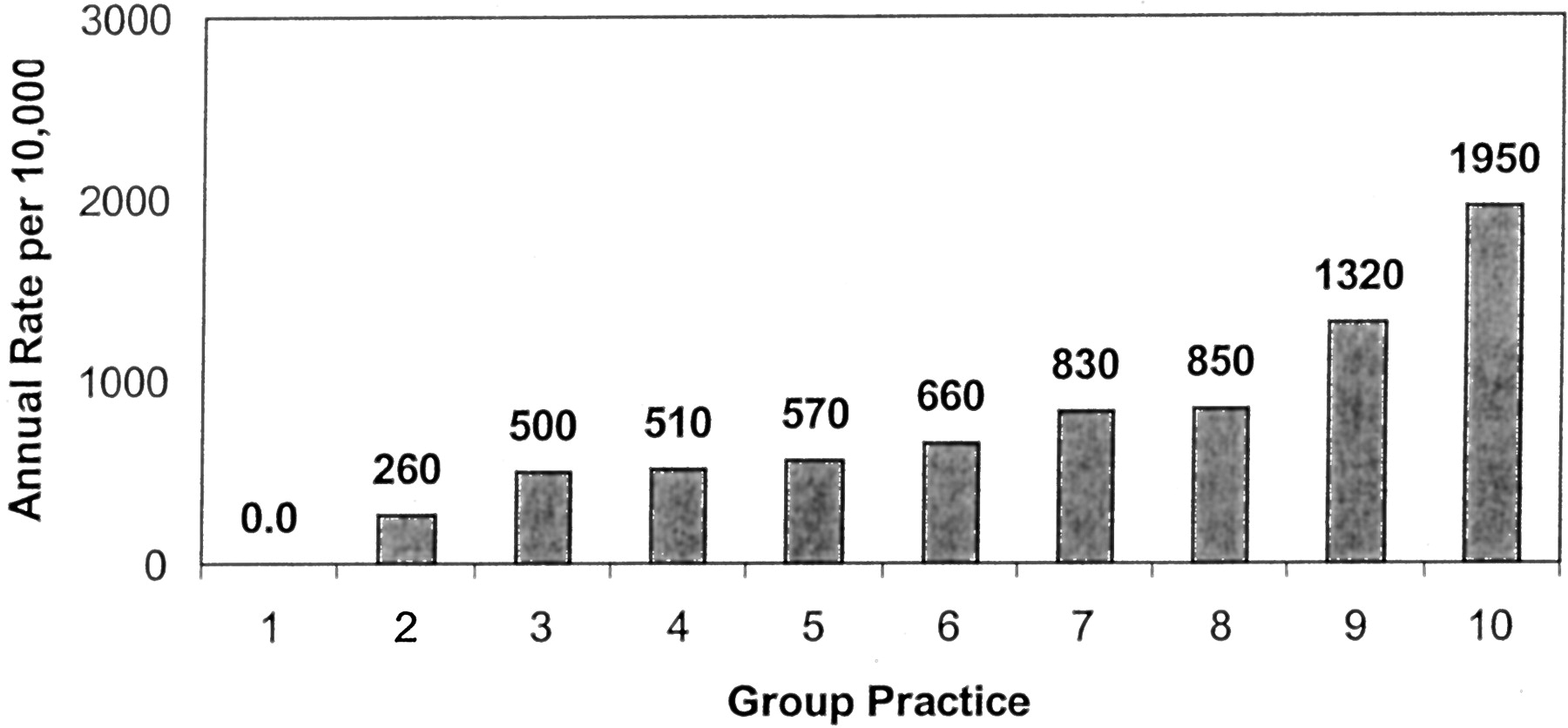
ER Utilization Rates for Asthma among Children on Medicaid in 10 Primary Care Practices
Results
The 2767 Medicaid-insured children (Table 1) generated 416 asthma-related billing events during the study period. Of these events, 196 ER visits (770 per 10,000 insured children) were made by 142 individual children. Within this group of children, 34 children (17%) had 2 or more visits. These 34 children accounted for 95 (49%) of all asthma-related ER visits by Medicaid insured children. Similarly, the 15 children (11%) with 3 or more ER visits accounted for 57 (29%) of all ER visits in this population. For the subset of children younger than 5 years of age, the rate of ER use was 1074 visits per 10,000 enrolled children.
Analysis showed that a primary care practice was assigned and could be identified for 2496 (90%) of all enrolled children. The 10 practices with 20 or more enrolled Medicaid children varied widely in the annual rate of emergency department visits for asthma from 0 to 1950 per 10,000 Medicaid-insured children (Figure 1). The heaviest rates were associated with urban practices, but no significant associations between practice characteristics and ER utilization for pediatric asthma could be made because of the small number of participating practices.
Mothers of 10 (75%) index children (one or more hospitalizations or at least 3 ER visits for asthma) confirmed intended participation in the focus groups and 6 (40% of all index children) actually attended. All were patients of the 3 practices with the highest rates of ER use.
The mothers expressed strong preferences for treatment at home or in the primary care clinic and regarded the ER as a “last resort” choice of care. Contacting physicians outside of office hours (after 5 pm on weekdays and throughout weekends) was identified as a primary problem. When physicians covering practices could be contacted after hours, parents were concerned about the quality of advice and lack of familiarity with the problems of the individual child. Mothers also reported difficulties in making appointments or being seen on an urgent basis by primary care physicians. Some physicians were perceived to create barriers to well-child visits for Medicaid-insured children but to allow unlimited ER visits. Mothers were unaware of Medicaid regulations concerning asthma management, including eligibility requirements for medication or devices and use of health services. Difficulties were reported in maintaining a consistent supply of prescription medications for asthma, primarily because of the need for physician approval of refills but also because of transport and logistic problems. Mothers reported receiving no preventive counseling concerning childhood asthma and little explanation of symptoms or education on the disease. The concept of case management was not familiar to the mothers, and they reported significant problems in the coordination of care between health providers. In most practices, standardization of treatment protocols was perceived to be lacking; the treatment provided at different visits varied considerably.
Although all parents of index children and most adult extended family members smoked, the focus group participants did not recall the impact of smoking being discussed or being offered effective smoking cessation interventions by primary care physicians. The mothers perceived the concept of home visits by asthma case managers positively, including using these visits to assist in obtaining asthma treatment services and in smoking cessation.
Discussion
As in studies of Medicaid-insured and Head Start children,9–12 members of health maintenance organizations,13 and inner-city communities,14,15 asthma was a common and serious health problem for Medicaid-insured children in Kansas. The estimated annual 1074 ER visits per 10,000 children under 5 years of age significantly exceeds the reported national average and makes the Healthy People Target of 80 per 10,000 seem unattainable by 2010. As reported in other studies, ER use was concentrated in a subgroup of children with half of all visits made by 17% of the Medicaid-insured children who used any emergency or hospital services for asthma.
Many aspects of asthma management depend on behavioral, cultural, and lifestyle factors. These factors may be invisible to health care researchers or providers because of educational, cultural, or socioeconomic differences between health professionals and patients. Qualitative research methods such as focus groups can identify patient perceptions of health problems and services, especially the motivations and logic behind health care decisions and actions.16 Focus groups are particularly useful in identifying barriers to health care access and understanding low rates of adherence with medical recommendations or treatment strategies. They have been used extensively to identify issues in low-income populations and groups with low literacy levels where conventional survey techniques are inappropriate and ineffective.17–19
The mothers in our focus group used ER services primarily because they perceived that primary care practices were not organized to meet the needs of their children with asthma. Besides difficulties in obtaining urgent advice or appointments, they frequently had difficulties in transport, childcare, or work release that impeded using the primary care office as the principal site of asthma care. In addition, practice organization and the episodic nature of asthma exacerbations resulted in little continuity of provider care for individual children, even if they used the primary care office. Exacerbating this problem, large group practices had no standardized protocols or consensus on asthma management leading to inconsistent advice and quality of care even within a single practice. About half of the mothers believed that the primary care physicians preferred patients to use the ER for acute asthma-related events.
The mothers’ experience with asthma care was largely limited to urgent visits during exacerbations of the illness. They were interested in working with case managers, including home visits, but were concerned about the ability of case managers to influence physician decisions and behavior. They were also interested in preventive measures, including smoking cessation, but none had been offered.
Conclusion
The decision to use ER services for childhood asthma in the Medicaid-insured population was driven by problems in using primary care services. The largest cluster of problems concerned accessing treatment for acute events, but the lack of preventive services was striking. Mothers of children who use ER services for asthma treatment regard this as a strategy of last resort and are interested in preventive measures, case management approaches, and increased use of primary care to manage their children’s asthma. Factors identified by mothers as currently limiting the management of childhood asthma in primary care include difficulty in obtaining urgent or convenient appointment, limited continuity of care, problems with after-hours coverage, lack of standardized, agreed management protocols and case management, and inattention to preventive measures. Many mothers reported an explicit or implicit encouragement of ER use by primary care physicians or their office staff members. This indicates that attention to aspects of practice organization, introduction of standardized management protocols, use of case managers, and attention to preventive measures, especially household tobacco smoke exposure, could significantly reduce ER use by Medicaid-insured children with asthma.
Significant effort has been made to prepare primary care practitioners to manage acute episodes of childhood asthma and institute preventive measures. Progress now depends on improved systems that enable physicians to care for Medicaid-insured asthmatic children in primary care practices. Further research to develop best practices and incentives is needed to overcome the current barriers for primary care physicians in managing Medicaid-insured children with asthma and in developing more effective partnerships between the parents/families of these children and health care professionals.
Notes
↵* Current affiliation: Anthem Blue Cross and Blue Shield, Richmond, Virginia.
- Received for publication July 25, 2003.
- Revision received July 25, 2003.





{kind=link}