
Abstract
Background: We examined whether physician compensation, financial incentives, and care management tools were associated with primary physician job and referral satisfaction. Our study was guided by a conceptual model of physician satisfaction derived from published evidence.
Methods: A cross-sectional survey was performed of 495 primary physicians (family practitioners, general practitioners, general internists) in the Seattle metropolitan area in 1997.
Results: Bivariate analyses revealed that salary compensation, productivity bonuses, and withholds for referrals were associated with job and referral dissatisfaction. However, after controlling for physician, practice, and office characteristics, only the association between salary payment and job dissatisfaction remained significant. Practice in offices with more physicians had the strongest association with physician job dissatisfaction.
Conclusions: Although managed care features are correlated with physician job and referral dissatisfaction, the source of dissatisfaction may originate from being an employed physician in a large medical group with more physicians, which may be more likely to impose bureaucratic controls that limit physician autonomy.
Many physicians believe that managed care and market competition have eroded their satisfaction with medical practice.1–9 Sources of physician dissatisfaction include loss of autonomy, increase in administrative burdens, potential loss of patients and income, greater time pressures, and threats of malpractice litigation.4,10–12
Physician satisfaction is important because it contributes to the quality of health care. Previous studies indicate that greater physician satisfaction is associated with appropriate prescribing practices,13 patient adherence,14 and greater patient satisfaction.15,16 Physician satisfaction also results in less turnover, which contributes to patients’ continuity of care, patient satisfaction and retention, and lower administrative costs of recruiting and replacing physicians.17,18 Dissatisfied physicians also may have more costly practice styles, generating more outpatient procedures and referrals.12 Because of these associations, provider satisfaction is regarded as 1 of the 4 critical outcomes of health care, along with health status, patient satisfaction, and cost.19
However, other studies report contradictory evidence about the relationship between managed care and physician satisfaction. For young physicians, managed care is not uniformly associated with less satisfaction.20,21 In 2 studies, HMO physicians had similar or greater satisfaction than physicians in fee-for-service practice,22,23 possibly because the clinical autonomy and income of the HMO physicians was satisfactory.3,9,18,23
Given the mixed evidence about the relationship between managed care and physician satisfaction, our aim was to determine whether physician compensation, financial incentives, and care management tools are associated with primary physician satisfaction. A related aim was to determine whether physician, practice, and office characteristics have stronger or weaker associations with primary physician satisfaction than managed care features.
Conceptual Model
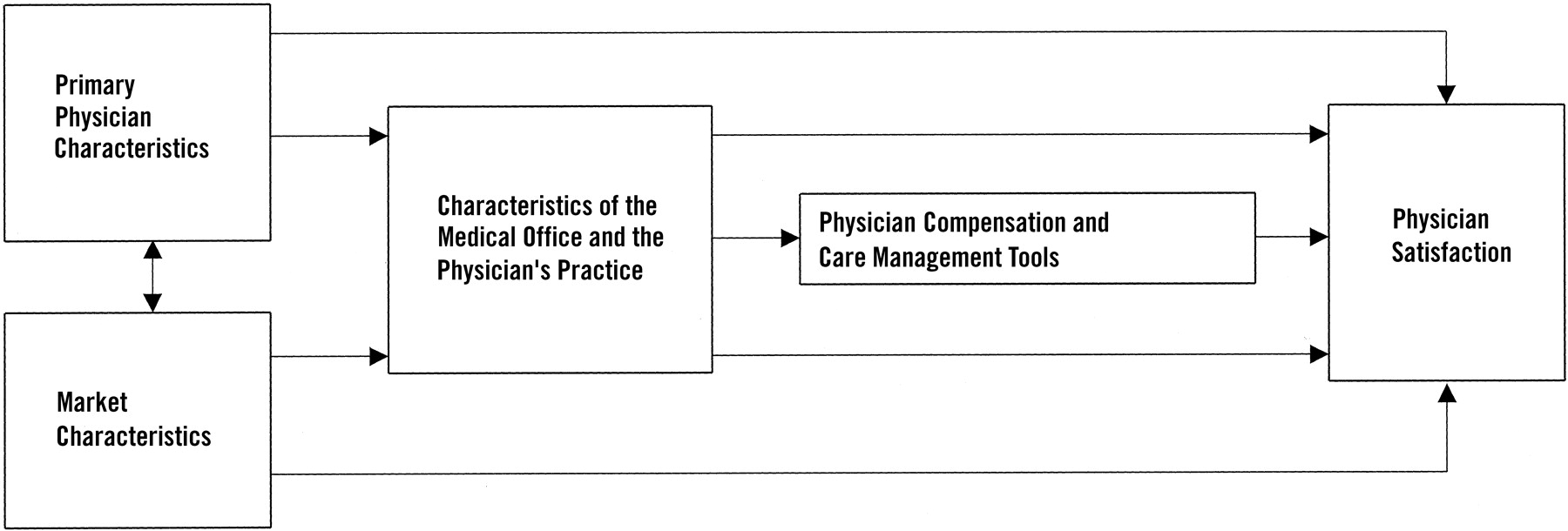
Figure 1 presents the conceptual model guiding our analysis of managed care and physician satisfaction, derived from Blumenthal et al24 and Hadley et al5 The figure itself is an extension of Reschovsky et al’s25 framework for examining managed care effects on physician perceptions of quality.

Conceptual model of physician satisfaction. Examples of primary physician characteristics include sex, specialty, board certification, and years in practice. Examples of market characteristics include the presence of managed health plans, penetration, and uninsured rate.
Reviewing Figure 1, the model posits that primary physician satisfaction is determined directly and indirectly by the characteristics of the market in which physicians practice, the characteristics of the primary physician, and the characteristics of the physician’s primary care office and its compensation and care management tools. A central assumption of the model is that primary physicians are not randomly allocated across primary care offices; rather, they select the offices in which they prefer to practice. In general, physicians seek offices having the right “balance” of bureaucratic autonomy (control over patient selection and time allocation) and clinical autonomy (control over patient care decisions).21,26,27 Some physicians prefer small, independent offices where they have both clinical and bureaucratic autonomy. Other physicians value larger group offices that have some bureaucratic structure, but doctors still control the use of tests and treatment selection. Physicians also tend to be more satisfied when their practices have fewer patients, less time pressure and stress, and greater resources.2,3,10,12,28–33
The choice of medical office largely determines physician compensation and the office’s tools for managing care, which are the “managed care features” of the model (see Figure 1). Physicians are more satisfied if compensated appropriately,28,32 although Williams et al30 found that income was unrelated to satisfaction. Physicians paid by salary were more dissatisfied than physicians paid by some form of fee-for-service,11 and physician payment based on productivity also was associated with dissatisfaction.30,34 Similarly, practice guidelines and protocols, which tend to be more common in HMOs, are associated with dissatisfaction,20 and the same relationship applies to financial and other incentives to reduce services.5,35 Physicians in medical groups with utilization management that restricts their autonomy were dissatisfied with patient care.4 These findings indicate that appropriate compensation and less managed care are associated generally with greater satisfaction.
We applied the model in Figure 1 to examine the associations between managed care and job and referral satisfaction among family physicians, general internists, and general practitioners in the Seattle metropolitan area.
Methods
Population
As part of our larger Physician Referral Study,36,37 we invited 832 primary physicians (family practitioners, general internists, and general practitioners) in private practice at least 50% of the time in the Seattle metropolitan area in 1997 to participate in the study. Of these, 261 physicians (31%) in 72 offices consented to participate. Participating physicians and a random sample of the primary physicians who did not participate (n = 300) were asked to complete self-administered questionnaires, which is the data source for this cross-sectional study.
Measures
Measures were chosen for 4 of the 5 components in the conceptual model (see Figure 1). Market characteristics were not measured because the study was conducted in a single market. The Seattle market had a relatively balanced mix of HMO, point-of-service, preferred provider organization, and fee-for-service health plans.37,38
Primary Physician Characteristics
Physician characteristics included gender, years in practice, and whether the physician was white or not. Specialty and board certification were measured using the American Medical Association Physician Masterfile.39 Physicians rated their tolerance for uncertainty in patient care by indicating agreement or disagreement with 2 statements: “the uncertainty of patient care often troubles me” and “uncertainty in patient care makes me uneasy.”40 Scores ranged from 2 to 8, where 8 indicates strong disagreement (ie, greater tolerance for uncertainty).
Medical Office and Physician Practice Characteristics
Office characteristics included office type (solo, primary group, or multispecialty group practice), the number of physicians in the office, and whether the office was owned privately. Physicians also rated how difficult or easy it was to refer a patient to a specialist on a 1-to-5 scale, where “1” indicates very difficult and “5” indicates very easy.
Physician workload was measured by patient visits per hour, administrative hours per week, and percentage of patients referred in a typical month. Patient mix was measured by the percentages of patients who were female, nonwhite, aged 18 and under, aged 65 and above, and from middle- or upper-class households.
Physician Compensation, Financial Incentives, and Care Management Tools
Physician compensation was measured by whether the physician was paid by salary or some form of fee-for-service. Financial incentives included whether the physician received a productivity bonus and had a financial withhold for referrals. Care management was measured in the following areas: financial risk (percentage of HMO patients in physician’s practice), utilization review (office prior approval required before referring patient to specialist inside or outside the office), and clinical guidelines (office follows written clinical guidelines for treating specific conditions or written referral guidelines for specific conditions).
Physician Satisfaction
Primary physician job satisfaction was measured with a 6-item scale adapted from adapted from Greenfield et al,41 and physician satisfaction with referrals was measured with a 3-item scale adapted from Shortell42 and Roulidis and Schulman,43 (Table 1). We measured physician satisfaction with referrals because referrals are part of everyday practice, a target of managed care controls, and a focus of our larger study. For each item, physicians rated their satisfaction on a scale of 1 (very dissatisfied) to 5 (very satisfied). Factor analysis of the 9 items revealed 2 groups consistent with the 2 scales. A physician’s job satisfaction was measured by averaging the 6 items in the scale, and physician referral satisfaction was defined the same way for the 3-item scale. The scales were correlated moderately (r = 0.37; P = .001), indicating the scales measured different dimensions of satisfaction.
Average Scores of Items in the Physician Satisfaction Scales (n = 498)
The physician job satisfaction scores had predictive validity. Physician satisfaction was measured in 1997; between 1997 and Fall 2000, we sent participating physicians periodic newsletters about the findings of the Physician Referral Study. The US Postal Service returned newsletters as “undeliverable/no forwarding address” for 44 physicians, which indicated physician turnover. We hypothesized that these physicians left their offices partly because of low job satisfaction.3,44 Analysis of variance (ANOVA) revealed that physicians who left their offices had less job satisfaction at baseline (3.39 average index score) than physicians who still received mail at office addresses (3.69 average index score; P = .016).
Data Collection
Data collection protocols were approved by the Human Subjects’ Internal Review Board at the University of Washington. The questionnaire survey was performed using methods developed by Dillman.45,46 The questionnaire, cover letter containing the elements of informed consent, postage-paid return envelope, and $20 incentive were inserted into a University of Washington “Husky” folder, and a token gift of appreciation was attached with ribbon to each folder. Study staff delivered the folders in person to the offices of participating and sampled nonparticipating primary physicians in the Seattle area. Nonrespondent physicians were sent a replacement questionnaire. Physicians who did not complete the replacement questionnaire were contacted by staff through telephone or fax to answer any questions about the study and draw their attention to the questionnaire.
Data Analysis
Bivariate ANOVA tests were computed to determine whether each physician, practice, office, compensation, and care management variable was associated significantly with physician job and referral satisfaction. For continuous variables, ANOVA tests were performed by dividing the distribution at the median.
Because associations between the care management variables and physician satisfaction could be caused by other variables in our conceptual model, multivariable statistical tests were conducted using partial correlation analysis. In the first analysis, we calculated the correlation between physician job satisfaction and each practice, office, compensation, and care management variable, controlling for physician characteristics. In the second analysis, we computed the correlation between physician job satisfaction and each office, compensation, and care management variable, controlling for physician and practice characteristics. Third, we computed the correlation between physician job satisfaction and each compensation and care management variable, controlling for physician, practice, and office characteristics. Fourth, we examined the partial correlation between physician job satisfaction and each physician, office, or care management characteristic, this time controlling for all other variables. Finally, we repeated these analyses for physician referral satisfaction.
We conducted both unweighted and weighted analyses based on the sampling fractions of the participating and nonparticipating physicians. Because the results were very similar, we present only the unweighted findings.
Results
About 97% of the participating physicians (n = 252) completed the self-administered questionnaire, and 81% of the randomly sampled, nonparticipating physicians (n = 243) completed their questionnaires. Results are based on 495 physician questionnaires. Physicians tended to be male, white, board-certified, and family practitioners (61%; Table 2). No statistically significant differences were detected between the job and referral satisfaction of participating versus nonparticipating physicians.
Characteristics Associated with Physician Job and Referral Satisfaction: Bivariate Results
Physician Job Satisfaction
Physician Compensation, Financial Incentives, and Care Management Tools
Bivariate results in Table 2 indicate that physicians were more dissatisfied when they were paid by salary than by fee-for-service, were paid a productivity bonus, and had a financial withhold for referrals. However, in multivariable models controlling for physician, office, and practice characteristics, only being a salaried employee was associated significantly with dissatisfaction across models (Table 3, top row).
Partial Correlations of the Determinants of Physician Job Satisfaction
Of the care management variables, bivariate results indicate that physicians were more dissatisfied when their offices required prior approval to refer to specialists outside the office (Table 2). However, this association disappeared when controlling for other characteristics (Table 3).
Physician Characteristics
Bivariate analyses indicate that physicians had greater job satisfaction if they were male, white, had less than 15 years of practice, and had greater tolerance for clinical uncertainty (Table 2). However, in multivariable analyses, tolerance for uncertainty was the only characteristic associated with greater job satisfaction (Table 3).
Practice Characteristics
Bivariate results reveal that physicians had greater job satisfaction if they worked fewer administrative hours, referred fewer patients, had more patients from middle- and upper-class households, and had fewer nonwhite patients (Tables 2 and 3). In multivariable analyses, only a single characteristic, fewer administrative hours, was associated consistently with greater satisfaction across models (Table 3).
Office Characteristics
In bivariate analyses, job satisfaction was highest for solo physicians, lowest for primary group physicians, and fell in between for physicians in multispecialty groups. Physicians were more satisfied in privately owned offices, in offices with fewer physicians, and offices in which it was easy to refer (Table 2). Controlling for physician and practice characteristics, the same associations were found. In multivariable analyses that controlled for all other variables (Table 3, right column), only 2 associations were found: fewer physicians in the office and ease of referral were associated with greater job satisfaction (partial r = −.24 and 0.20, respectively). The smaller number of associations may be a result of correlations among the office characteristics (for example, multispecialty group practices generally had more physicians than other practices).
Physician Referral Satisfaction
Physician Compensation, Financial Incentives, and Care Management Tools
In bivariate analyses, physicians who had a financial withhold for referrals were more dissatisfied with referrals (Table 2). However, this association was not significant in multivariable models controlling for practice and office characteristics (Table 4). Although a greater percentage of HMO patients and absence of a productivity bonus were associated with greater referral satisfaction (Tables 2 and 4), these associations were not significant after controlling for other characteristics (Table 4).
Partial Correlations of the Determinants of Physician Referral Satisfaction
Physician, Practice, and Office Characteristics
In bivariate analyses, referral satisfaction was highest for solo physicians, lowest for primary group physicians, and in-between for physicians in multispecialty groups. Physicians had greater referral satisfaction if they had more years of practice, had greater tolerance for uncertainty, worked fewer administrative hours, owned the practice, and thought it was easy to refer (Tables 2). In multivariable analyses, only 2 characteristics, ease of referral and greater tolerance for uncertainty, were associated consistently with greater referral satisfaction across models (Table 4).
Discussion
For primary physicians in the Seattle area, physician compensation, financial incentives, and care management tools were not associated generally with physicians’ job and referral satisfaction. Bivariate analyses revealed initially that being a salaried employee, productivity bonuses, and withholds for referrals were associated with job and referral dissatisfaction. However, after controlling for physician, practice, and office characteristics, only the association between salary payment and job dissatisfaction remained significant.
Changes in physicians’ practice arrangements may explain these findings. As managed care and market competition grew in the 1990s, so did the prevalence of group practices.47–49 Many primary physicians shifted—sometimes reluctantly—from solo to group practice and from being owners to being salaried employees.49 Compared with solo practice, large medical groups are more likely to be bureaucratic and to impose controls on the clinic and workload autonomy of their physician employees, mainly to reduce costs and improve quality of care.34,48
The impact of these practice changes on physician job satisfaction are reflected in our results. We found that primary physicians are more dissatisfied in offices with a greater number of physicians, in group rather than solo offices, and when they do not own the practice. When we controlled for these office characteristics in multivariable analyses, financial incentives (a productivity bonus and referral withholds) were no longer associated with dissatisfaction, which suggests that the office characteristics are the source of the dissatisfaction. Salary payment was still associated with dissatisfaction, perhaps because employee physicians in group offices had less autonomy, and because this form of compensation limited physician incomes. These findings are consistent with our conceptual model (Figure 1).
We also found that care management tools were not associated with job or referral satisfaction. The finding is consistent with evidence that care management tools, by themselves, have little influence on practice behavior.50
Administrative hours, ease of referral, and tolerance of uncertainty also are determinants of physician satisfaction. Greater administrative hours, an indicator of bureaucratic medicine that may be associated with greater stress, was associated with physician job dissatisfaction, which is consistent with past studies. Ease of referral was associated with greater job and referral satisfaction. We suspect that ease of referral may be a proxy indicator for a “well-run” office that helps physicians practice medicine, manages their patient flows, and respects their clinical autonomy. Physicians with greater tolerance for uncertainty in patient care also have greater job and referral satisfaction, which is consistent with Freeborn’s study of Kaiser Permanente physicians.12 Tolerance for uncertainty may be an important “buffer” that helps physicians cope with the inherent uncertainty of patient care, as well as managed care controls targeting physicians’ clinical decisions.
Understanding the sources of physician dissatisfaction is important because dissatisfaction may have adverse effects on the cost, quality, and outcomes of care.35 Salaried employment in large medical groups may be a risk factor for physician dissatisfaction. In these settings, physician dissatisfaction can be reduced by installing administrative arrangements that protect clinical autonomy and offer reasonable work schedules and compensation.18,26 Similarly, physician job and referral satisfaction may be increased through medical school curricula and continuing education that increase tolerance for uncertainty in daily practice. This is particularly important with the growth of evidence-based medicine, which may actually increase the complexity of patient care and therefore the importance of this competency.51,52
Limitations
Our findings are limited to primary physicians in Seattle in 1997, and relationships between managed care and physician satisfaction may be different in other places and periods. Our results may be influenced by nonresponse to the physician survey, but the relatively low nonresponse rate reduces this problem. Our data are cross-sectional, and associations between variables may not be causal. Because our data come from a single market, we cannot examine the association between market characteristics and physician satisfaction. We did not measure all aspects of physicians’ offices and practices that might be associated with physician satisfaction.
Conclusions
Office managed care was generally not associated with physician job or referral satisfaction. Of the physician compensation, financial incentive, and care management variables that we examined, only being a salaried employee was associated with physician job dissatisfaction. The number of physicians in the medical office had the strongest association with physician job dissatisfaction. These findings imply that the source of dissatisfaction is being an employed physician in a large medical group, which may be more likely to impose bureaucratic controls that limit physician autonomy. Primary physicians may have greater job satisfaction in smaller, less bureaucratic offices that protect their autonomy in work schedules and clinical decision-making.
Notes
This work was supported by grant HS11712 from the Agency for Healthcare Research and Quality.
- Received for publication August 2, 2002.
- Revision received August 2, 2002.
REFERENCES




{kind=link}
Jump to section
Related Articles
Cited By...
- Staff perceptions of community health centre team function in Ontario
- What keeps family physicians busy in Portugal? A multicentre observational study of work other than direct patient contacts
- Quality of Work Life of Independent vs Employed Family Physicians in Wisconsin: A WReN Study
- Time Spent in Face-to-Face Patient Care and Work Outside the Examination Room